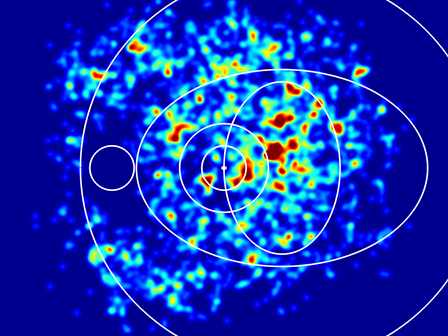
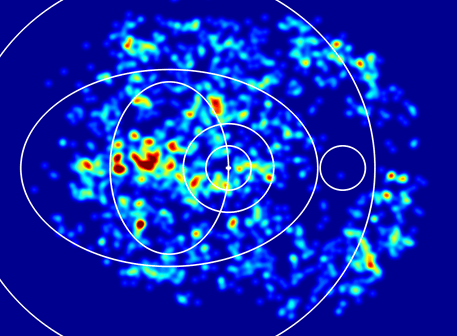
Distribution of miicroanreurisms of the dataset
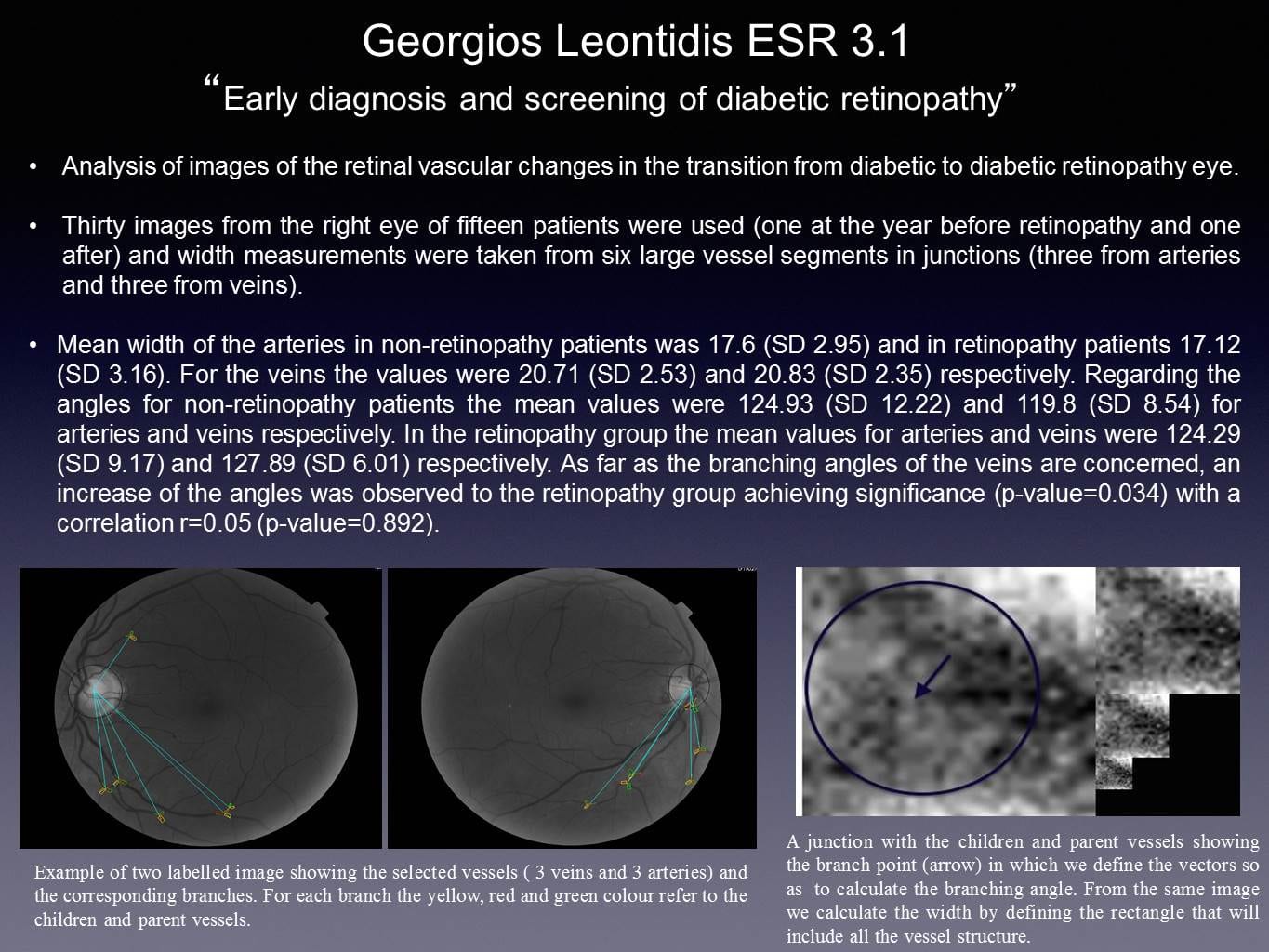
Number and location of lesions for the optimisation of the screening interval in diabetic retinopathy
Diabetic retinopathy is a leading cause of blindness in the Western World. The disease is detected by screening which includes visual acuity measurement and fundus photography (Stefansson et al. 2000; Jeppesen & Bek 2004; WHO 2008; Bandello et al 2013). On the basis of the diabetes type and the severity of retinopathy a fixed interval to the following screening examination defined to ensure that no patient will develop vision threatening complications during that period (Singer et al. 1992; AAO Diabetic Retinopathy PPP 2012). However, this rule-based approach also implies that patients with slow disease progression will experience a number of superfluous examinations without consequences for the management of the disease. A reduction in the number of these examinations requires an algorithm that considers the patient’s individual risk factors (Aspelund et al 2011). The inclusion of risk factors such as sex, age at onset of diabetes mellitus, diabetes type, diabetes duration, HbA1c and blood pressure has been shown to allow a significant prolongation of the control interval without increasing the risk of developing vision threatening retinopathy (Mehlsen et al. 2012). The predictive value of this model was found to be lowest for patients with more severe retinopathy, and it was concluded that the grader might have included other factors than the severity of retinopathy in the decision, such as the location of retinopathy lesions or conditions unrelated to diabetic retinopathy (Hove et al. 2004, 2006). Therefore, 81 patients out of 6868 observations where the prediction of the model matched exactly or deviated significantly (3 or more time intervals) from the clinician’s recommended interval were identified. The fundus photographs documented during the screening visits from these patients were reviewed in order to investigate the role of the location of retinopathy lesions and the role of the presence of retinal lesions unrelated to diabetic retinopathy in the assessment of control intervals of the same or different lengths in time, whether assessed using the rule based approach or the individualised model.